Measles: Clinical Features and CDC Recommendations

SUMMARY:
- Measles (Rubeola)
- Caused by an RNA virus with 1 serotype
- Humans are the only natural hosts of measles virus
- Average of 10 to 12 days from exposure to the appearance of the first symptom (usually fever)
- Healthcare providers should report suspected measles cases to their local health department within 24 hours
- Groups at high risk for severe illness include
- Infants and children aged <5 years
- Adults aged >20 years
- Pregnant women
- People with compromised immune systems, such as from leukemia and HIV infection
KEY POINTS:
- Clinical Features
- Measles Transmission
- Complications
- Diagnosis and Testing
- Evidence of Immunity
- Measles Vaccine Recommendations (CDC)
- Post-exposure Prophylaxis
- Isolation
- Treatment
- Measles and Pregnancy
- Contraindications and Precautions
Clinical Features
- Typical presenting features
- Prodrome of fever (as high as 105°F) and malaise
- The 3 ‘C’s: Cough | Coryza (runny nose) / Conjunctivitis
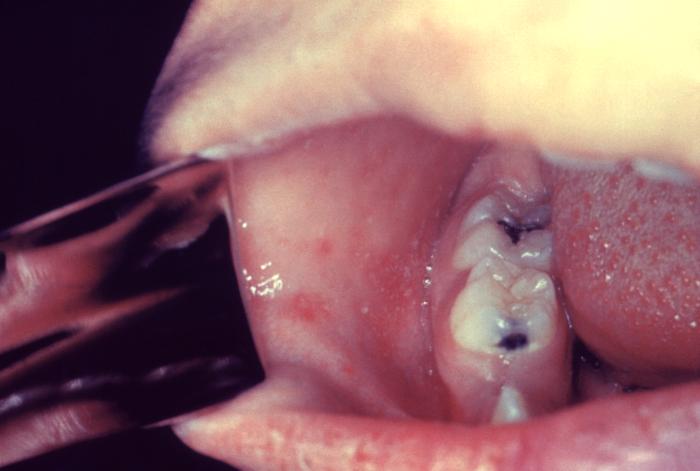
- 2 to 3 days: Pathognomonic enanthema: Koplik spots within 2 to 3 days
- white spots with red areola on buccal mucosa across from lower molars
- 3 to 5 days: Maculopapular rash
- Appears 14 days after a person is exposed
- Spreads from the head to the trunk to the lower extremities
- Patients contagious from 4 days before to 4 days after the rash appears
- Note: Immunocompromised patients may not develop rash

Measles Transmission
- Individuals are contagious from 4 days before to 4 days after the rash appears
- Considered an ‘highly contagious virus’ according to CDC
- “…if one person has it, up to 90% of the people close to that person who are not immune will also become infected”
- Virus lives in nose and throat mucus of an infected person
- Spread via
- Breathing contaminated air: Virus can live in an airspace where the infected person coughed or sneezed for up to 2 hours
- Touching infected surface: Followed by touching eyes, nose or mouth
Complications
- Common complications include
- Bronchopneumonia | Laryngotracheobronchitis | Diarrhea
- Otitis Media: 1/10 children and may result in permanent hearing loss
- Severe complications in children requiring hospitalization
- Acute encephalitis: 1/1,000 children, resulting in permanent brain damage
- Respiratory and neurologic: 1/1,000 children will die from these complications
- Subacute sclerosing panencephalitis (SSPE): Rare, fatal degenerative disease of CNS, resulting in deterioration and seizures 7 to 10 years after measles infection
Diagnosis and Testing
- Clinical suspicion
- Signs and symptoms detailed above
- Special concern for those traveling internationally or exposed to someone with a febrile rash illness
- Laboratory confirmation
- Essential for all sporadic measles cases and all outbreaks
- A capture IgM EIA (non-quantitative) that incorporates a recombinant measles nucleocapsid protein as the antigen is used to detect measles IgM
- A commercial, indirect EIA (non-quantitative) assay is used to detect IgG
- Viral detection methods: Includes real time RT-PCR to detect measles viral RNA | Available at many state public health laboratories and though the APHL/CDC Vaccine Preventable Disease Reference Centers (see ‘Learn More – Primary Sources’ below)
- Detection of measles-specific IgM antibody in serum and measles RNA by RT-PCR in a respiratory specimen are the most common methods for confirming measles infection
- Obtain both a serum sample and a throat swab (or nasopharyngeal swab) from patients suspected to have measles at first contact
- Urine samples may also contain virus: If possible collect both respiratory and urine samples
- Public Health: Molecular analysis (genotyping) can map transmission pathways of measles viruses
Evidence of Immunity
Note: Do not accept verbal reports of immunity
Acceptable presumptive evidence of immunity against measles includes ≥1 of the following
- Written documentation of one or more doses of a measles-containing vaccine administered on or after the first birthday for preschool-age children and adults not considered high risk
- Written documentation of two doses of measles-containing vaccine for school-age children and adults at high risk, including students at post-high school secondary educational institutions, healthcare personnel, and international travelers
- Laboratory evidence of immunity *
- Laboratory confirmation of measles
- Birth before 1957
*Note: CDC addresses laboratory evidence of immunity and states the following
*People who have negative or equivocal results for measles IgG should be vaccinated or revaccinated. In some cases it is not possible to vaccinate a patient, and you may need to test them with a second line diagnostic assay to determine whether they are immune to measles. Because the sensitivity and specificity of commercial measles IgG assays vary, state public health departments can provide information on appropriate second line assays.
NOTE FOR HEALTHCARE PERSONNEL (HCP): CDC has interim guidance that states
Consider vaccinating HCP born before 1957 who do not have other evidence of immunity to measles
During a measles outbreak, 2 doses of measles virus-containing vaccine are recommended for all HCP, regardless of year of birth
See more HCP interim guidance using the CDC link below in ‘Learn More – Primary Sources’
Measles Vaccine Recommendations (CDC)
- Children – MMR vaccine
- First dose: 12 through 15 months of age
- Second dose: 4 through 6 years of age no earlier than 28 days following the first dose
- Students at post-high school educational institutions without evidence of measles immunity
- 2 doses of MMR vaccine
- Second dose administered no earlier than 28 days after the first dose
- Adults born ≥1957 who do not have evidence of measles immunity
- Should get at least one dose of MMR vaccine
- International travelers ≥6 months of age
- Infants 6 through 11 months: one dose of MMR vaccine
- One dose at 12 through 15 months of age and another dose at 4 through 6 years of age or at least 28 days later
- Infants who get one dose of MMR vaccine before their first birthday should get two more doses according to the routinely recommended schedule
- Children ≥12 months: Documentation of two doses of MMR vaccine (the first dose of MMR vaccine should be administered at age 12 months or older; the second dose no earlier than 28 days after the first dose)
- Teenagers and adults born ≥1957 (no immunity): Documentation of two doses of MMR vaccine, with the second dose administered no earlier than 28 days after the first dose
- Infants 6 through 11 months: one dose of MMR vaccine
Post-exposure Prophylaxis
Cannot Readily Show Evidence of Immunity Following Exposure to Measles
- Offer post-exposure prophylaxis (PEP) or be excluded from the setting (school, hospital, childcare)
- Unvaccinated individuals who receive their first dose of MMR vaccine within 72 hours after exposure may return to childcare, school, or work except healthcare workers
- PEP: Administer MMR vaccine within 72 hours of initial measles exposure or immunoglobulin (IG) within six days of exposure
- Monitor for signs and symptoms consistent with measles for at least one incubation period following PEP
- Note: “Do not administer MMR vaccine and IG simultaneously, as this practice invalidates the vaccine”
MMR vaccine for PEP
- Should still offer MMR vaccine even if beyond 72 hours to protect from future exposures
- Outbreak control measure for infants <12 months of age: Measles vaccination of infants as young as 6 months of age may be used (revaccinate when they are 12 through 15 months old and again when they are 4 through 6 years of age)
Immunoglobulin (IG) for PEP
- IG dosing
- IGIM dose: 0.5 mL/kg of body weight (maximum dose = 15 mL)
- IGIV dose: 400 mg/kg
- IG used for high risk populations
- Pregnant women without evidence of measles immunity
- Intravenous IG (IGIV)
- Severely compromised immune systems
- Administer IGIV regardless of immunologic or vaccination status
- Note: People cannot return to healthcare settings following receipt of IG | For other settings, such as childcare, school, or work “factors such as immune status, intense or prolonged contact, and presence of populations at risk, should be taken into consideration before allowing people to return”
- Pregnant women without evidence of measles immunity
- PEP for healthcare personnel
- MMR vaccine should be given within 72 hours or IG should be given within 6 days
- “Exclude healthcare personnel without evidence of immunity from duty from day 5 after first exposure to day 21 after last exposure, regardless of post-exposure vaccine”
Isolation
- Isolate for four days after they develop a rash
- Use airborne precautions in healthcare settings
- All healthcare staff entering the room should use respiratory protection consistent with airborne infection control precautions (use of an N95 respirator or a respirator with similar effectiveness in preventing airborne transmission)
- Use single-patient airborne infection isolation room (AIIR) for patient with measles
- People without evidence of immunity who have been exempted from measles vaccination for medical, religious and now PEP within appropriate timeframe
- Exclude from affected institutions in the outbreak area until 21 days after the onset of rash in the last case of measles
Treatment
- There is no specific antiviral therapy for measles
- Supportive care to address symptoms and complications
- Severe measles in children: Administer Vitamin A (a substrate for preserving epithelial cell integrity and involved in immune modulation) immediately on diagnosis and repeated the next day with following dosing
- <6 months: 50,000 IU
- 6–11 months: 100,000 IU
- ≥12 months: 200,000 IU
Measles and Pregnancy
- Pregnant women are considered a ‘high risk’ category due to increased risk for adverse maternal, fetal and newborn events
- Maternal: Increased risk of hospitalization and severe respiratory complications including pneumonia
- Fetal: Miscarriage | Stillbirth | LBW | Preterm birth
Prior to Pregnancy
- Ensure vaccinations are up to date
- Wait 4 weeks following MMR to conceive
- Theoretical risk, not proven and should not be used as an indication for termination of pregnancy (if vaccine received inadvertently)
During Pregnancy
- CDC recommends that pregnant women should wait to get MMR vaccine until after they are no longer pregnant
Postpartum
- Give MMR postpartum if no evidence of immunity
- Breastfeeding is safe and does not impact vaccine
Contraindications and Precautions to MMR Vaccine
Contraindication – Greatly Increases Chance of Serious Adverse Reaction
The following individuals should not receive MMR vaccine
- History of severe allergic reaction (e.g., anaphylaxis) following previous dose or to a vaccine component
- Known severe immunodeficiency
- Pregnancy (see above re: theoretical risk)
- History of anaphylactic reactions to neomycin
Precaution – Might increase the chance or severity of a serious adverse reaction or might compromise the ability of the vaccine to produce immunity
Precautions for MMR vaccine include the following
- Moderate or severe acute illness with or without fever
- Recent (within 11 months) receipt of antibody-containing blood product (timing depends on product)
- History of thrombocytopenia or thrombocytopenic purpura
- Need for tuberculin skin testing
- Personal or family history of seizures
Learn More – Primary Sources:
CDC: Measles Cases and Outbreaks
CDC: Measles (Rubeola) for Healthcare Professionals
Vaccine Preventable Diseases (aphl.org)
CDC: Routine Measles, Mumps, and Rubella Vaccination
CDC: Interim Infection Prevention and Control Recommendations for Measles in Healthcare Settings
